

TL;DR: Hyperbaric chambers increase dissolved oxygen in your blood plasma under pressure, triggering measurable physiological responses. Whether that translates into a meaningful benefit depends on chamber type, pressure level, oxygen delivery, session count, and use context. Most published evidence comes from clinician-supervised medical HBOT using hard-shell systems, and that evidence should not be automatically transferred to home or general wellness chambers. Casual wellness claims are often broader than the data supports.
There’s a steel tube in the corner of a growing number of wellness centers, pro athlete recovery rooms, and suburban garages. Inside: you, lying flat, breathing oxygen while pressure climbs. Outside: a lot of conflicting information about whether this thing does anything worth the money.
Let’s sort it out. No hand-holding.
What Pressurized Oxygen Actually Does to Your Body
You know the basic pitch. Pressurized chamber, more oxygen, body responds. The part most people skip is why pressure matters more than the oxygen itself.
Under normal conditions, hemoglobin is already carrying oxygen at roughly 97% saturation. You can’t load much more onto those trucks. What pressure does is bypass the trucks entirely. It dissolves oxygen directly into your plasma, cerebrospinal fluid, and lymphatic fluid—changing how oxygen is transported, not just how much rides on hemoglobin.
Henry’s Law governs this. Double the pressure, roughly double the dissolved oxygen. At 2.0 ATA breathing 100% oxygen, dissolved plasma oxygen reaches levels far above what you get at normal atmospheric pressure. Reviews of HBOT mechanisms have confirmed that pressurized oxygen increases the proportion of dissolved oxygen in blood by multiple-fold depending on the pressure applied. [1,2]
In published research—especially higher-pressure, clinician-supervised protocols—that physiological state has been associated with downstream effects such as:
- Capillary formation — repeated sessions have been associated with signaling involved in new capillary network development
- Stem cell release — some studies suggest bone marrow-derived stem cells can increase in peripheral circulation after repeated sessions
- Inflammatory modulation — certain inflammatory markers may shift under specific protocols
- Mitochondrial support — oxygen availability can improve ATP production in stressed cells
- Antimicrobial support — hyperoxic environments can enhance oxygen-dependent immune activity under certain conditions
None of this is magic. It’s gas physics meeting cell biology. But the combination is more sophisticated than most marketing copy lets on.
Hyperbaric Chamber Evidence: Where It’s Strong and Where It’s Not
Not everywhere. And not all chambers, protocols, or use cases belong in the same bucket. Here’s the honest map:
| Context | What the Research Actually Reflects | Strength of Evidence |
|---|---|---|
| Clinician-supervised medical HBOT | This is where the strongest published evidence sits: hard-shell systems, higher pressures, controlled oxygen delivery, defined protocols, and medical oversight | Strong for medical HBOT in its own clinical context |
| Brain, cognition, and inflammation-related research | There is growing literature, but outcomes vary substantially with protocol design, pressure, oxygen delivery, and session count | Mixed to promising |
| Athletic recovery | Subjective fatigue sometimes improves; objective physical recovery markers are less consistent across studies | Mixed |
| General wellness optimization | Claims tend to run ahead of the evidence, especially when the promise is broad and the goal is vague | Limited |
| Soft-shell and home-use systems | Accessibility is better, but controlled published research is far thinner than the literature on medical HBOT | Limited |
That’s the part that gets blurred in marketing. The strongest evidence is evidence for specific protocols, in specific settings, with specific equipment—not a blanket endorsement of every chamber on the market.
Where It’s Just Noise
Pressurized oxygen is not a shortcut, not a substitute for appropriate care, and not a license to promise everything from sharper focus to total-body transformation. The regulatory line matters. Product type matters. Intended use matters. The claims made around the chamber matter.
That distinction isn’t bureaucratic nitpicking. It determines whether you’re looking at a real intervention with defined parameters or a broad lifestyle promise wrapped in science language.
Hyperbaric Chamber Types: Soft-Shell vs. Hard-Shell — What You’re Actually Getting
This is the conversation most articles avoid because it’s commercially inconvenient. But it matters.
| Feature | Soft-Shell Chamber | Hard-Shell Chamber |
|---|---|---|
| Pressure range | 1.3–1.5 ATA; some models claim up to 1.95 ATA | 1.5+ ATA |
| Oxygen delivery | Ambient air or concentrated O₂ via mask, often around 90–95% | 100% medical-grade oxygen, chamber-pressurized or mask-delivered |
| Construction | Inflatable polyurethane or reinforced nylon; zipper seal | Rigid steel or medical-grade acrylic; pressure-locked |
| Portability | Can deflate, relocate, fit in a spare bedroom | Fixed installation; may require structural planning |
| Where published evidence comes from | Very limited compared with hard-shell literature | Nearly all peer-reviewed HBOT research |
| Best suited for | Home wellness routines, accessibility, and lower-pressure use | Clinician-supervised HBOT and higher-dose protocols |
The honest takeaway: soft-shell and hard-shell chambers are different products delivering different doses. A 2024 review found that hyperbaric treatment at 1.5 ATA can increase blood and tissue oxygen and activate measurable cellular responses. That’s meaningful. But the step from 1.3 ATA with ambient air to 2.0 ATA with 100% oxygen isn’t linear—it’s a different intervention category. Most published protocols documenting robust physiological changes use defined pressures and high-concentration oxygen in hard-shell systems. 3
That doesn’t mean soft-shell units are worthless. It means the outcomes from one don’t automatically transfer to the other, and anyone telling you otherwise isn’t being straight with you.
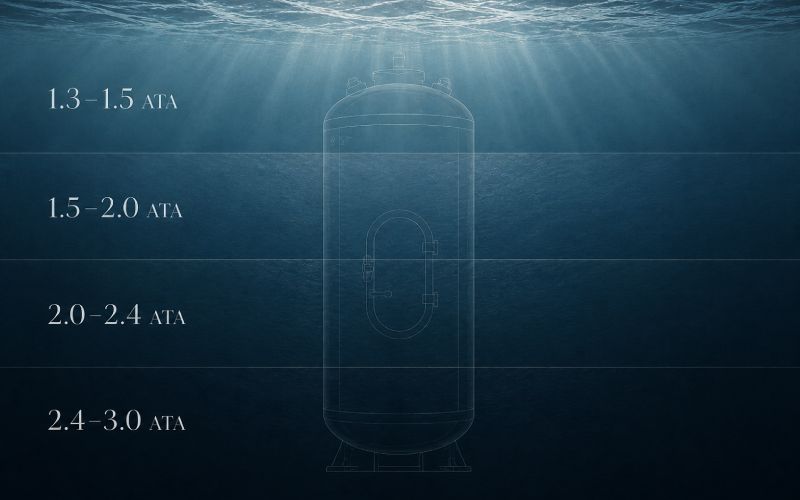
Hyperbaric Chamber Pressure Levels: What Each One Does
| Pressure (ATA) | Equivalent Depth | Typical Session | Primary Context |
|---|---|---|---|
| 1.3 – 1.5 | ~10–16 feet underwater | 60–90 min | Home wellness, entry-level recovery, lower-pressure use |
| 1.5 – 2.0 | ~16–33 feet | 60–90 min | Frequently studied range in published HBOT research |
| 2.0 – 2.4 | ~33–46 feet | 45–90 min | Common range for clinical HBOT protocols |
| 2.4 – 3.0 | ~46–66 feet | 40–60 min | Advanced protocols requiring supervision |
Higher isn’t automatically better. A 2023 systematic review and meta-analysis found that adverse effects were more likely when chamber pressure exceeded 2.0 ATA, while pressures below 2.0 ATA had a relatively lower side-effect profile. Choosing a pressure level should be driven by context, equipment, and protocol—not by the assumption that more equals better. 4
Hyperbaric Chamber Side Effects and Safety
The side effect profile can be manageable under appropriate protocols, but this is not a zero-risk environment. Pressure is real. Oxygen is real. Safety rules exist for a reason.
Common:
- Ear discomfort from pressure equalization, the airplane landing feeling
- Temporary nearsightedness
- Mild fatigue or headache after sessions, especially early ones
- Sinus pressure in people with congestion
Uncommon:
- Temporary worsening of certain eye conditions
- Claustrophobia-related anxiety
Rare but serious:
- Oxygen-toxicity events under certain conditions
- Lung irritation from prolonged, repeated high-oxygen exposure
- Fire risk in oxygen-enriched environments
One commonly cited absolute contraindication in HBOT literature is an untreated pneumothorax. Beyond that, cautions can apply depending on respiratory status, recent surgery, medications, pregnancy, and the broader clinical picture. And if you’re dealing with a specific symptom, diagnosis, or recovery issue, that moves the conversation out of casual wellness and into professional evaluation. FDA has also emphasized following device instructions, fire prevention measures, training, supervision, and maintenance for HBOT devices. [5,6]
How Sessions Actually Work
You lie down in a tube or sit in a room. The chamber pressurizes over 10–15 minutes. You equalize your ears. Pressure stabilizes. You breathe. You wait.
Sessions typically run 60–90 minutes at pressure. Many protocols include air breaks—short intervals breathing normal air—to reduce oxygen toxicity risk. Decompression takes another 10–15 minutes. You get up, you leave.
Most studied protocols involve repeated sessions over days or weeks. The time commitment is significant and usually glossed over by people selling the experience as casual wellness.
The effects are cumulative. One session produces a temporary spike in dissolved oxygen. Repeated sessions are what published protocols actually study. Expecting transformation from three sessions is like expecting fitness from three gym visits.

FAQ
Does one session do anything noticeable?
Some people report feeling clearer or more energized after a single session. But the more meaningful changes discussed in published research are generally tied to repeated exposure, not one-off novelty. One session is an experience. A protocol is an intervention.
How do I know if my situation is one where pressurized oxygen might actually help?
Start with this: are you asking a general wellness question, or are you trying to address a specific symptom, condition, or recovery issue? That distinction matters. The strongest evidence in this space comes from defined protocols in defined settings—not a generic promise that any chamber works for any goal.
What’s the real difference between soft-shell and hard-shell chambers?
Soft-shell chambers usually operate at lower pressures and often use concentrated oxygen or ambient air. Hard-shell chambers can reach higher pressures with 100% medical-grade oxygen. They’re not interchangeable interventions at different price points—they’re different doses of different setups.
Can pressurized oxygen help with athletic recovery?
Possibly. Some research and plenty of athlete anecdotes point to reduced perceived fatigue or better recovery rhythm. But the evidence is narrower than the marketing, and objective performance or recovery markers are not uniformly improved across studies. Think additive, not transformative. [7,8]
Is there anyone who absolutely should not use a hyperbaric chamber?
Untreated pneumothorax is commonly treated as a hard stop in HBOT literature. Beyond that, this becomes a case-by-case question involving respiratory status, medications, recent procedures, pregnancy, and overall risk profile. That’s exactly why broad wellness marketing can only take this conversation so far.
How many sessions will I need?
There is no universal number that honestly covers every chamber, every goal, and every protocol. Published research is all over the map. What matters is the match between the equipment, the pressure, the session design, and the goal.
The Honest Answer
Pressurized oxygen changes physiology. Demonstrably. Measurably. In specific contexts.
What is not honest is pretending that all chambers, all pressures, all oxygen delivery methods, and all use cases belong in the same sentence. They don’t.
The chamber isn’t hype when it’s discussed with precision: what kind of chamber, what pressure, what oxygen source, what protocol, what goal, what setting. It becomes hype the moment someone starts collapsing all of that into one glossy claim.
Know what you’re buying. Know what the published evidence actually reflects. And know the difference between the tube and the marketing around it.
References
1 Ortega MA, Fraile-Martínez O, García-Montero C, et al. “A General Overview on the Hyperbaric Oxygen Therapy: Applications, Mechanisms and Translational Opportunities.” Medicina, 2021. (PMC)
2 Lindenmann J, Smolle C, Kamolz LP, Smolle-Juettner FM, Graier WF. “Survey of Molecular Mechanisms of Hyperbaric Oxygen in Tissue Repair.” International Journal of Molecular Sciences, 2021. (MDPI)
3 Cannellotto M, Yasells García A, Landa MS. “Hyperoxia: Effective Mechanism of Hyperbaric Treatment at Mild-Pressure.” International Journal of Molecular Sciences, 2024. (Springer)
4 Zhang Y, Zhou Y, Jia Y, Wang T, Meng D. “Adverse effects of hyperbaric oxygen therapy: a systematic review and meta-analysis.” Frontiers in Medicine, 2023. (PubMed)
5 U.S. Food and Drug Administration. “Follow Instructions for Safe Use of Hyperbaric Oxygen Therapy Devices — Letter to Health Care Providers.” August 25, 2025. (U.S. Food and Drug Administration)
6 Gawdi R, et al. “Hyperbaric Oxygen Therapy Contraindications.” StatPearls / NCBI Bookshelf, updated 2025. (National Center for Biotechnology Information)
7 Gušić M, et al. “Effects of hyperbaric oxygen therapy on recovery after a football match in young players: a double-blind randomized controlled trial.” Frontiers in Physiology, 2024. (Frontiers)
8 Luo X, et al. “Effects of Hyperbaric Oxygen Therapy on Exercise-Induced Muscle Injury and Soreness: A Systematic Review and Meta-analysis.” Archives of Physical Medicine and Rehabilitation, 2025. (ScienceDirect)
This content is for informational and educational purposes only. It is not intended to diagnose, treat, cure, prevent, or address any specific condition, and it should not be read as medical advice or as a statement of intended medical use for any product. Always follow the manufacturer’s instructions for use and consult an appropriate qualified professional when evaluating any specific symptom, condition, or safety question.