
Disclaimer: This article discusses the physics and general physiology of mild hyperbaric pressure environments (1.3–1.5 ATA) for wellness purposes only. Nothing here is medical advice. The devices discussed on this site are not intended to diagnose, treat, cure, or prevent any disease.

You step inside what looks like a large zippered capsule. The door seals. A quiet hiss begins. And from there, physics takes over.
That’s the short version. But the longer explanation behind how a mild hyperbaric chamber actually works is worth understanding — and most write-ups either oversimplify or overcomplicate. Let’s try to land somewhere useful.
The Core Idea: Pressure Changes How Oxygen Behaves
A mild hyperbaric chamber is a sealed enclosure that raises air pressure around your body — modestly, to about 1.3 to 1.5 times normal atmospheric pressure. That shift changes the way oxygen moves through your bloodstream.
Under everyday conditions, oxygen travels through blood mostly by binding to hemoglobin molecules inside red blood cells. About 97–98% of blood oxygen moves this way 1. The remaining small fraction dissolves directly into blood plasma — the liquid portion of your blood.
Here’s where the chamber does its thing. When ambient pressure increases, more oxygen molecules get pushed into that plasma. Not metaphorically. Literally. The gas dissolves into the liquid at a higher rate.
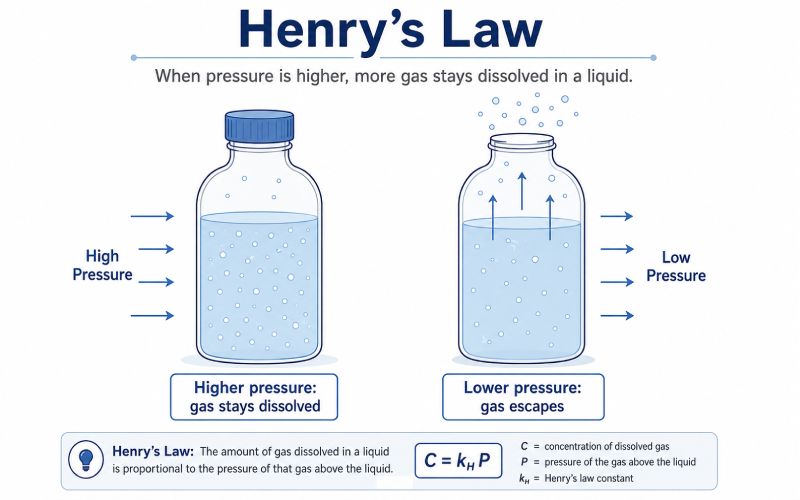
This is governed by Henry’s Law — the amount of gas that dissolves in a liquid is directly proportional to the pressure of that gas above the liquid [2].
Think of a sealed carbonated drink. Carbon dioxide stays dissolved while the cap is on and pressure is high. Open it, pressure drops, bubbles rush out.
A mild hyperbaric chamber does the reverse. It keeps the cap on tighter.
Henry’s Law in Your Bloodstream
Henry’s Law sounds academic, but what it describes is straightforward. Gas wants to escape liquid. Pressure prevents that escape. More pressure, more gas stays dissolved.
In your blood, this plays out in a measurable way. At normal sea-level pressure (1.0 ATA), plasma carries a small amount of dissolved oxygen — roughly 0.3 mL per 100 mL of blood [2]. That’s because hemoglobin handles nearly all the oxygen-carrying work 1.
Raise the pressure to 1.3 or 1.5 ATA while breathing enriched oxygen from a concentrator, and that dissolved oxygen number climbs meaningfully.
The math is simple. Dissolved oxygen in plasma follows a linear relationship: for every 1 mmHg increase in the partial pressure of oxygen in the blood, roughly 0.003 mL of additional oxygen dissolves per 100 mL of plasma [2]. Sounds tiny — until you realize that a mild chamber with enriched oxygen pushes partial pressure from around 100 mmHg to somewhere between 600 and 900 mmHg.
| Condition | Pressure | Approx. Dissolved O₂ (per 100 mL blood) | vs. Baseline |
|---|---|---|---|
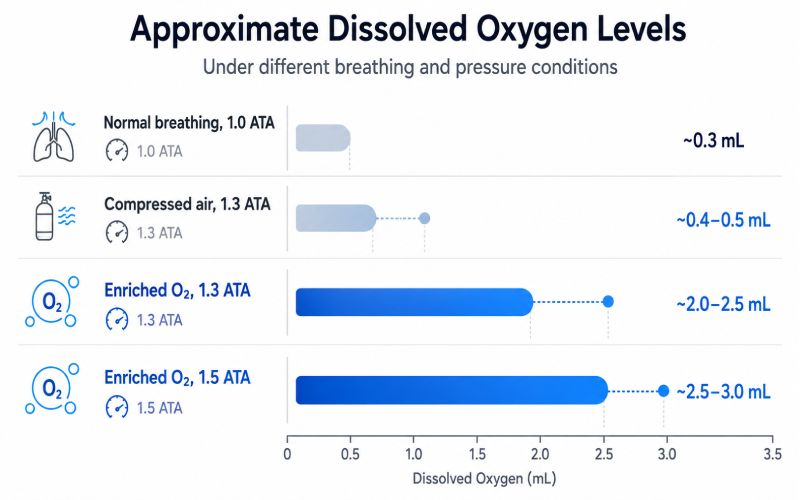
| Normal breathing at sea level | 1.0 ATA | ~0.3 mL | — |
| Mild chamber, compressed air only | 1.3 ATA | ~0.4–0.5 mL | ~1.5× |
| Mild chamber + enriched O₂ (~93%) | 1.3 ATA | ~2.0–2.5 mL | ~7–8× |
| Mild chamber + enriched O₂ (~93%) | 1.5 ATA | ~2.5–3.0 mL | ~8–10× |
Values are approximate. Individual results vary with physiology, altitude, and equipment output. Calculations based on published oxygen solubility coefficients [2].
Even at the lower end — 7× baseline — that represents a real change in how much oxygen circulates freely in liquid form, available to reach cells throughout the body.
What Happens Inside Your Body During a Session
Step by step:
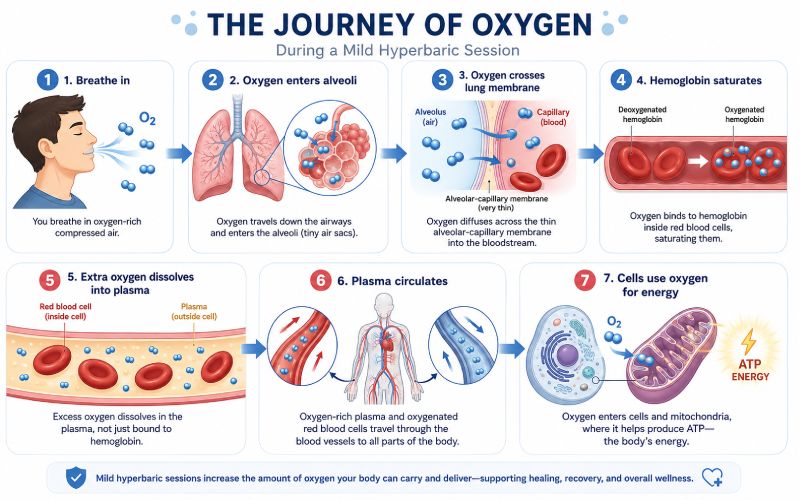
1. You breathe in. Same as always. Air enters the lungs, fills the alveoli — the tiny air sacs where gas exchange occurs.
2. Oxygen crosses the lung membrane. O₂ molecules move from the alveoli into surrounding capillaries through diffusion — from higher partial pressure to lower [3].
3. The pressure difference matters here. Because the chamber has raised ambient pressure, the partial pressure of oxygen in the alveoli is higher than it would be in a normal room. That steeper gradient drives more oxygen across the membrane and into the blood [3].
4. Hemoglobin picks up what it can. Red blood cells grab oxygen. But hemoglobin is already nearly full under normal conditions — about 97% saturated 1. Low ceiling. You hit it fast.
5. Surplus oxygen dissolves into plasma. This is the key mechanism. Under increased pressure, oxygen that hemoglobin can’t carry dissolves directly into the liquid plasma. Henry’s Law, doing what Henry’s Law does [2].
6. Oxygen-rich plasma circulates. Plasma flows everywhere blood goes. The dissolved oxygen it carries diffuses into surrounding cells, supporting normal oxygenation and the body’s everyday energy processes.
7. Cells use the oxygen. Oxygen fuels mitochondrial energy production — the process that generates ATP, the molecule behind most cellular work. More dissolved oxygen available means cells can maintain efficient energy output more easily.
Physics influencing biology. Nothing more mysterious than that.
Why Not Just Breathe More Oxygen Without the Pressure?
This question comes up a lot. And it’s a good one.
You can breathe higher concentrations of oxygen at normal atmospheric pressure. Some wellness setups offer this. And yes, it does raise blood oxygen — slightly.
But the effect has a hard limit.
Hemoglobin is already near maximum at 97% saturation under regular conditions 1. Breathing richer oxygen at 1.0 ATA might push that to 99 or 100%. Marginal gain.
The actual bottleneck is plasma solubility. At normal pressure, plasma can’t hold much dissolved gas. The molecules escape — same way carbonation leaves a loosely capped bottle.
Pressure is the variable that changes the equation. By increasing atmospheric pressure inside the chamber, you push oxygen to dissolve into plasma at quantities that aren’t achievable at 1.0 ATA. That’s why the chamber needs to be sealed and pressurized in the first place.
Without the pressure, you’re breathing richer air. With it, you’re changing the physics of gas transport in your blood.
What It Feels Like Inside
Not dramatic. Really.
When pressurization starts, you hear a quiet hissing. Temperature may rise a few degrees — compressed air warms up because compression increases gas temperature, which is what happens when gas gets compressed in a confined space [4]. Your ears will likely feel full, same as on an airplane during ascent. Swallowing or yawning usually handles it.
Once the chamber reaches target pressure — 1.3 to 1.5 ATA — the ear sensation fades. Breathing feels completely normal. Most people relax, nap, read, or listen to something. There’s no tingling, no rush, no obvious sign that dissolved oxygen levels in your plasma have changed. Your body doesn’t register it consciously.
At the end of a session, pressure gradually releases. Some ear popping. Air cools slightly. Some people feel relaxed or drowsy afterward — a combination of the oxygen exposure and an hour of stillness.
The whole experience is passive. You sit, breathe, and the chamber handles the physics.
Why the Pressure Changes Slowly
Pressurization isn’t instant. Chambers ramp up over 10 to 15 minutes. This gives your body time to equalize — particularly the air-filled spaces in your ears and sinuses. Rushing it causes discomfort, so the gradual approach is part of the design.
Depressurization follows the same logic. Slow return to normal. If pressure dropped too fast, dissolved gases could theoretically form small bubbles — the same principle that makes gradual ascent important in scuba diving. At 1.3–1.5 ATA, this risk is essentially nonexistent. But controlled speed remains standard anyway.
The session arc: slow ramp up → sustained pressure → slow ramp down.
Useful oxygen absorption happens during the sustained middle phase. That’s why most sessions run 60 to 90 minutes — enough time at pressure for the dissolved oxygen effect to accumulate and circulate.
Quick Recap
- Chamber seals → pressure rises to 1.3–1.5 ATA.
- Partial pressure of oxygen increases → more O₂ per breath.
- Lungs absorb more oxygen → steeper diffusion gradient.
- Hemoglobin saturates → hits its ~97% ceiling quickly.
- Surplus dissolves into plasma → Henry’s Law.
- Plasma circulates freely → delivers dissolved O₂ body-wide.
- Cells use the oxygen → supports natural energy production.
- Session ends → pressure returns to normal gradually.
Pressure in. Oxygen dissolves. Pressure out. That’s the whole thing.
FAQ
Does higher pressure always mean better? Not in a linear way. Mild chambers at 1.3–1.5 ATA already produce a meaningful increase in dissolved plasma oxygen, especially with enriched air. The relationship isn’t “more pressure, more benefit” without limit — it’s about matching pressure to your goals and your equipment’s design range.
How quickly does oxygen dissolve once pressure stabilizes? Fast. Plasma oxygen levels begin rising within minutes of reaching target pressure. The sustained session time allows that oxygen-rich plasma to circulate thoroughly.
Why does the chamber warm up? Compressing gas increases temperature [4]. The temperature rise is modest and usually fades once full pressure is reached.
Can you feel the extra oxygen? Not directly. No rush, no tingling. Effects tend to be subtle and cumulative — supporting natural recovery after exercise, more consistent energy — noticed over days or weeks of regular use.
What does ATA mean? Atmospheres absolute. It measures total pressure including the normal atmosphere. Sea level is 1.0 ATA. A chamber at 1.3 ATA applies 30% more pressure than sea level.
Is the oxygen inside the chamber pure? Most mild chambers use concentrators delivering approximately 93% oxygen. The remaining ~7% is mostly nitrogen. Even at this purity level, the dissolved oxygen increase at 1.3–1.5 ATA is substantial — as the table above shows.
References
- Collins, J.A., Rudenski, A., Gibson, J., Howard, L., & O’Driscoll, R. “Relating oxygen partial pressure, saturation and content: the haemoglobin–oxygen dissociation curve.” Breathe, 11(3), 194–201, 2015. doi:10.1183/20734735.001415. Link
- Pittman, R.N. “Oxygen Transport.” In: Regulation of Tissue Oxygenation. San Rafael, CA: Morgan & Claypool Life Sciences, 2011. Link
- Treacher, D.F. & Leach, R.M. “Oxygen transport—1. Basic principles.” BMJ, 317(7168), 1302–1306, 1998. doi:10.1136/bmj.317.7168.1302. Link
- NASA Glenn Research Center. “Compression and Expansion.” Beginners Guide to Aeronautics. Link